


Winters may be getting milder overall, but climate change is fueling more intense and disruptive storms, putting worker health and safety at greater risk when cold weather hits.



This article is part of the National Commission on Climate and Workforce Health’s series “Climate Prescription.”
Written by Dr. Leah B. Topper, a family medicine physician and Climate & Health Science Policy Fellow at the University of Colorado School of Medicine, the series translates the latest research on climate-driven health risks into practical insights for employers, HR leaders, and workplace health professionals.

Since I moved to North Carolina, winter has generally been milder. The two snowstorms we experienced in January, however, were a surprise for North Carolinians. The intensity of the storms led to clinic closures, school cancellations, and road conditions that kept many people home for days.
As a family medicine physician, I found myself fielding questions not just about colds and flu, but about medication access and what to do in case of a power outage.
These extreme weather events are a reminder that our changing climate is causing wide-ranging health and safety challenges.
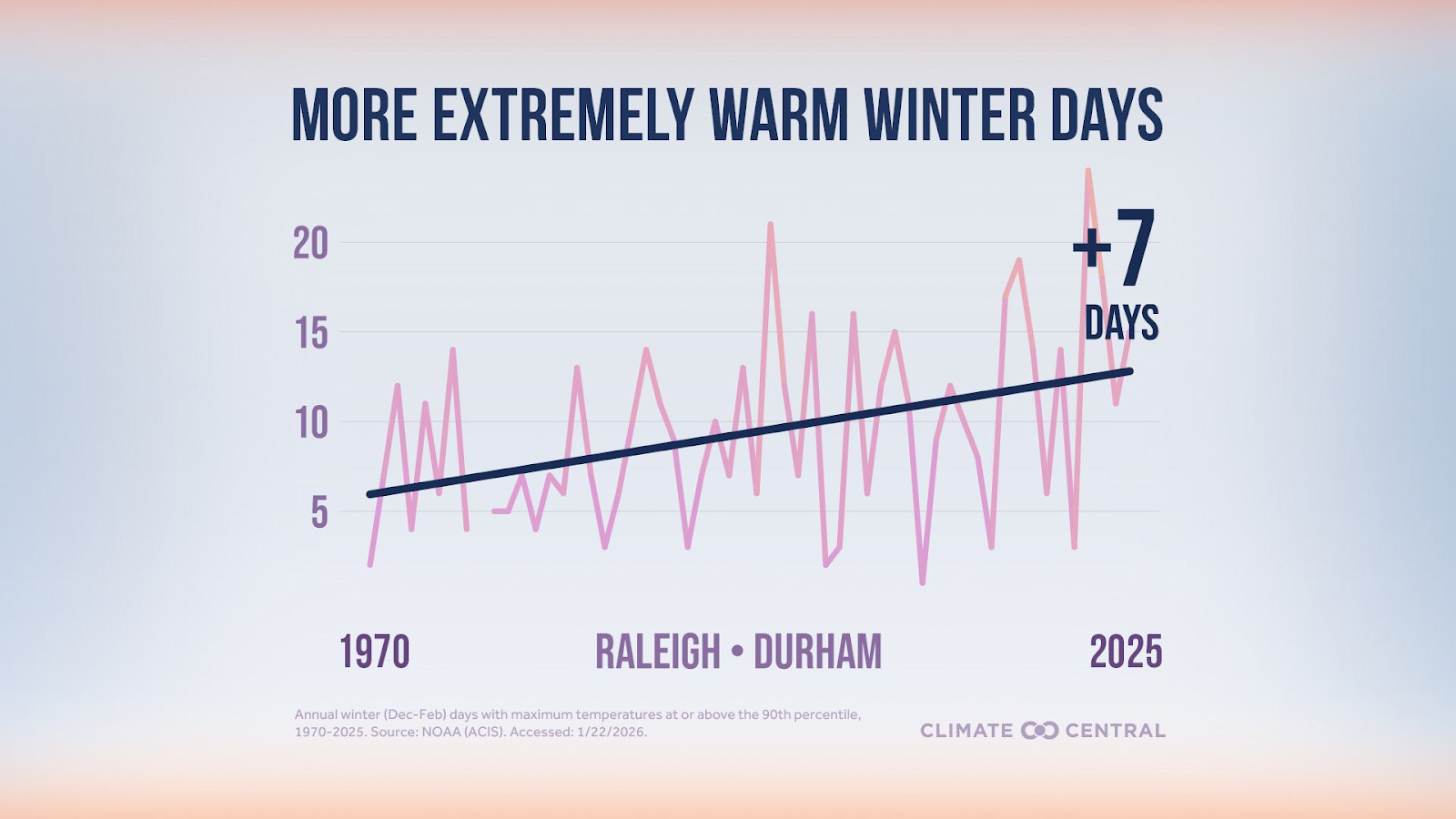
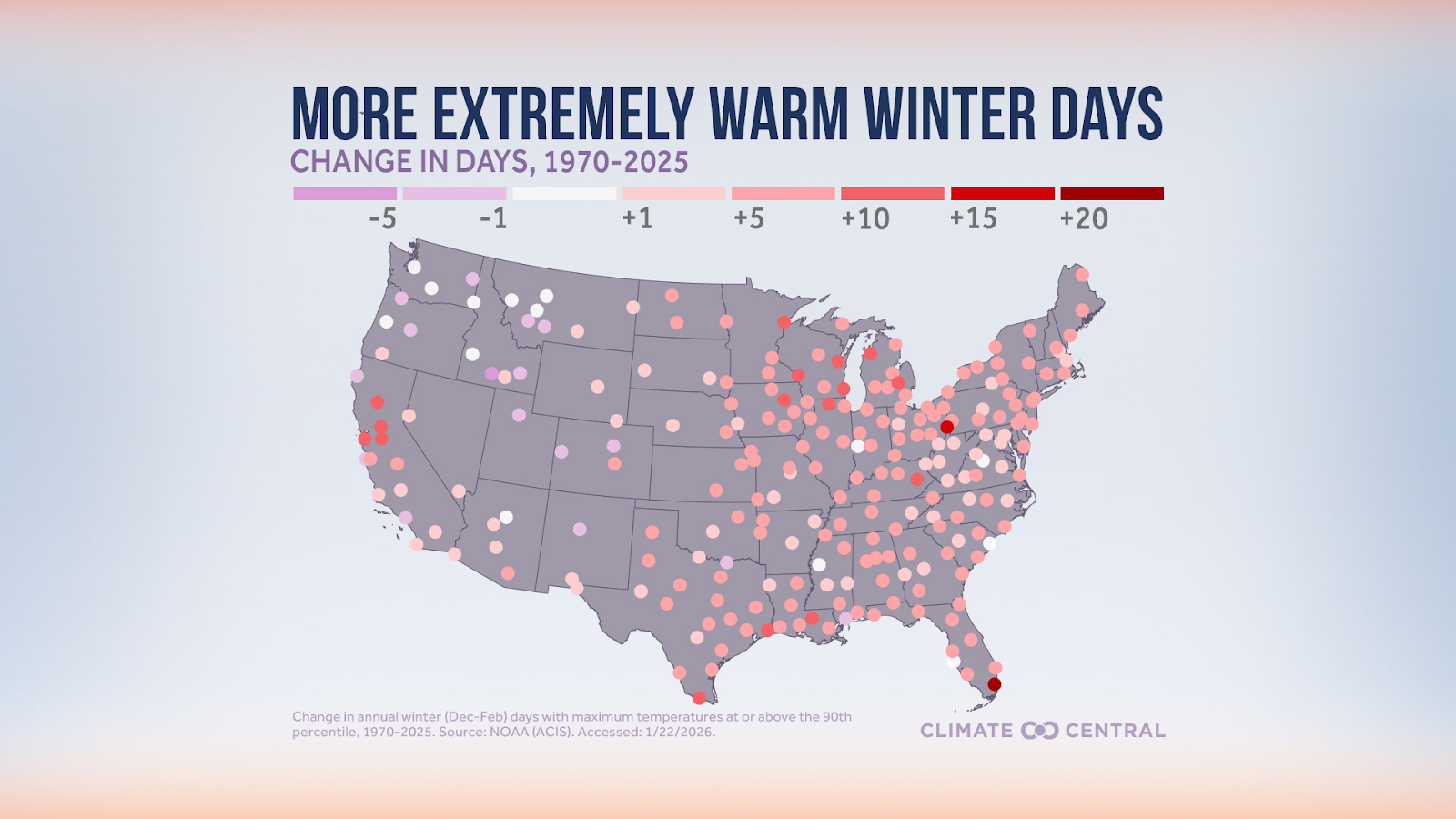
Winter is the fastest-warming season across much of the United States. On average, that has meant less snow in most places; but even as our atmosphere warms overall, we see heavier snowfall in certain regions. Climate Central found that nearly two-thirds of U.S. locations now receive less snow than in the early 1970s, while about one-third receive more.
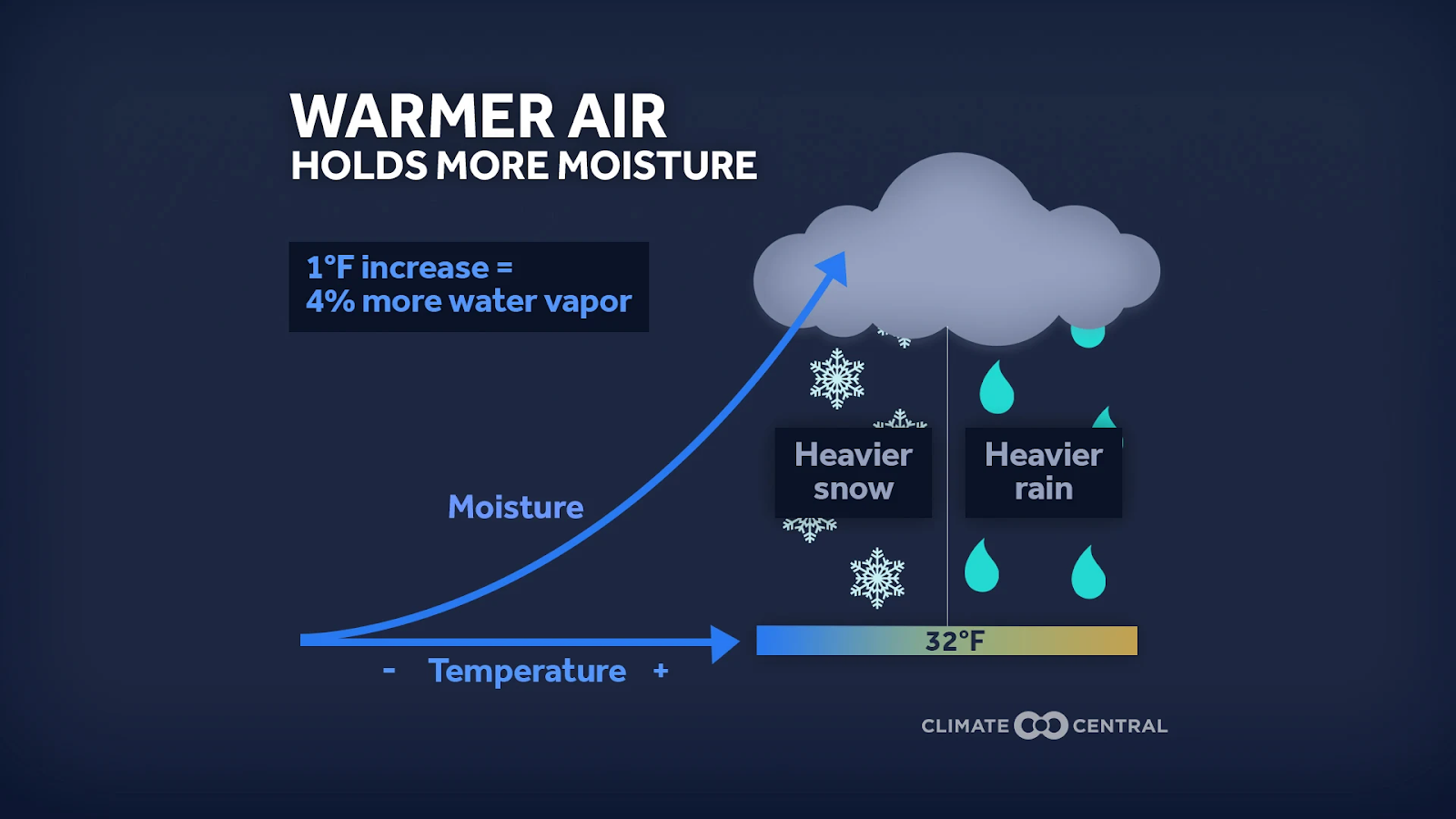
How can both be true? Warmer air holds more moisture. When temperatures dip below freezing, that moisture can fall as heavy snow when conditions are right. Changes in freeze-thaw cycles, stronger winds, and increased atmospheric moisture contribute to less-predictable winters — milder overall, but punctuated by intense winter storms. Furthermore, warmer temperatures can make winter storms more dangerous when the higher moisture-containing air is not frozen into snow, instead falling as sleet and freezing rain.
From a health perspective, extreme winter storms are a serious environmental stressor.
The most directly cold-related illnesses are hypothermia and frostbite, but many other health effects are less obvious. We see increased rates of asthma and COPD due to cold, dry air, which irritates the airways. People generally spend more time indoors during the winter, often in small, confined spaces, increasing transmission of respiratory infections such as influenza, COVID-19, and RSV.
Specific types of injuries are also associated with winter weather. Fall-related emergency department visits have been shown to increase during inclement winter weather. Specific types of bone fractures have been correlated with the winter season. Studies have even shown an increase in heart attacks following exposure to cold weather.
Indoor environments pose their own risks. Indoor air quality may be poor during the wintertime due to reduced ventilation to keep heat in, which can increase exposure to particulate matter and volatile organic compounds. Poor air quality can worsen lung and heart conditions as well. Power outages are also more likely during severe winter weather, and people often turn to alternative heating sources, increasing the risk of carbon monoxide poisoning.
Finally, there is the psychological toll. Severe winter storms can cause isolation, disrupted routines, and uncertainty, amplifying stress, anxiety, and depression.
I am grateful that most of my patients navigated these recent storms safely. Patients who rely on electricity for medical equipment had backup power plans or were able to relocate temporarily. Those concerned about access to essential medications due to road or pharmacy closures were able to refill their prescriptions before the storms. Ultimately, the storms were less severe than anticipated, and widespread power loss did not occur in the areas where my patients live.
But that outcome was not guaranteed. That's why preparation and prevention are integral and prioritized over reactive solutions.
Clinically, health care conversations regarding extreme winter weather increasingly include:
These same principles apply beyond the exam room.
For employers, winter storms are a health and safety issue, as well as an operational challenge. Fatalities associated with winter storms are rarely caused by the storm itself; they are far more often due to car accidents, hypothermia, or delayed medical care. Roughly one-quarter of weather-related vehicle crashes occur on snowy, slushy, or icy pavement, and 15% happen during snowfall or sleet.
To better prepare, employers can:
While heat-related illness often dominates the conversation, the effects of climate change on winter should also be acknowledged. When a heavy winter storm hits, it may cause more unpredictability, variability, and disruption to infrastructure.
As a family physician, my role is to help patients anticipate risks and prioritize their health and safety. As employers, neighbors, and family, we share responsibility for creating systems that prioritize preparation, communication, and adaptability to respond to future extreme winter weather events.


Want to help your company adapt to today’s climate conditions and invest in human and business resilience? Sign up for our monthly newsletter to stay up to date on the latest events, resources, and recommendations from the National Commission on Climate and Workforce Health.


The National Commission on Climate and Workforce Health is a group of business, health, and climate leaders who share a mission to protect workers from the health risks posed by extreme weather.
The Commission was created by the Health Action Alliance in partnership with Mercer and with strategic input from the CDC Foundation. Additional support for the initiative is being provided by The Hartford. Learn more at ClimateHealthCommission.org.

Sign up for our newsletter to keep updated on HAA’s latest initiatives, insights and recommendations, and be first to receive new resources and event invitations.
Sign up


.svg)